Healthy Tazewell County Initiative: Variations in Community Quality of Life, Health Problems, and Risky Behaviors by Age Category
Alyssa Carlson
Angela Stegmaier
Maureen Cluskey*
G. Kevin Randall*
Bradley University
Key Words: community health, Mobilization for Action Through Planning and Partnerships (MAPP), and age category.Abstract
The MAPP process, a strategic planning tool that allows communities to prioritize their public health issues, was employed by the Tazewell County Health Department to assess what factors residents perceived to be (a) the most important for community quality of life, (b) the greatest health problems, and (c) the top risky behaviors impacting community health.
Data, collected through an online survey, were provided by 456 participants residing in the county and at least 18 years of age. First, we conducted a frequency analysis on the top three factors for community quality of life, health problems, and risky behaviors as nominated by participants. Second, we assessed whether or not the factors differed by age groups/cohorts: 25-34, 35-44, 45-55, 55-64, and those over 65.
Although the top factors for community quality of life did not vary much by age cohort, 38 percent of those 65+ listed religious or spiritual values as one of their top three. Heart disease and stroke were common health concerns, but the youngest group listed teen pregnancy as a top health concern (35.6%), whereas the three older groups cited health problems associated with aging as a concern. The groups agreed consistently on the top three risky behaviors.
Thus for these survey respondents, the top factors for community quality of life, and the top health problems varied by age category. Implications for public policy are discussed, including how age cohort related issues such as religiosity and health problems impact constituency preferences.
Introduction
Public health aims to improve the wellbeing of a population through disease prevention and increased health awareness (Diclemente, Crosby, & Kegler, 2009; Stover & Bassett, 2003). To recognize problems and determine corrective action, research must be conducted to show disparities in health and quality of life (Israel, Schultz, Parker, & Becker, 1998). Community-based public health research focuses on finding these disparities and improving quality of life through the active involvement of community members, researchers, and organizations (Israel et al., 1998; Norris & Pittman, 2000).
To conduct this research, programs and collaborative partnerships have been formed (Bakes-Martin, Corso, Landrum, Fischer, & Halverson, 2005). The Mobilization for Action Through Planning and Partnerships (MAPP) process is an example of such a program. Created by the National Association of County and City Health Officials (NACCHO) in alliance with the Public Health Practice Program Office, and the Centers for Disease Control and Prevention (CDC), MAPP is a strategic planning tool that allows communities to prioritize public health issues, find strengths and gaps within communities, and improve upon them (McClellan, 2005).
Using MAPP's six steps, (a) Organizing, (b) Visioning, (c) Assessments, (d) Identify Strategies, (e) Formulate Goals and Strategies, and (f) Action, The Tazewell County Health Department employed the MAPP process to assess what factors residents perceived to be the most important for community quality of life, the greatest health problems, and the top risky behaviors impacting the community. Existing literature has examined the factors citizens perceive as the most important qualities of life within communities (Oates, 2012). However, there is a lack of information regarding how age may influence the factors an individual believes make up a healthy community.
Due to possible age related differences in perception, our study investigated the factors that make up a healthy community, and separated respondents by age category to identify how different generations viewed these components. It is thought that several different aspects make up an individual's subjective age. For instance, chronological age may impact an individual's perception of certain health problems depending on their stage within the lifespan; this is due to certain age groups being at a higher risk for chronic disease or other age-related health concerns. Therefore, because certain life events and experiences are more prominent in different age groups, they play a role in variations of age identity (Monetpare, 2009). Thus, it was hypothesized that the top three factors for community quality of life, health problems, and risky behaviors would differ based on the age category of the respondents.
Method
Sample and Procedures
Data, collected through an online survey, were provided by 456 participants residing in the county and at least 18 years of age. First, we conducted a frequency analysis on the top three factors for community quality of life, health problems, and risky behaviors as nominated by participants. Second, we assessed whether or not the factors differed by age groups/cohorts: 25-34, 35-44, 45-55, 55-64, and 65 and over.
Measures
Age Categories. Respondents were stratified by self-reported age: 25-34 years (n=59); 35-44 years (n=84); 45-55 years (n=107); 55-64 years (n=112); and 65 years and older (n=94).
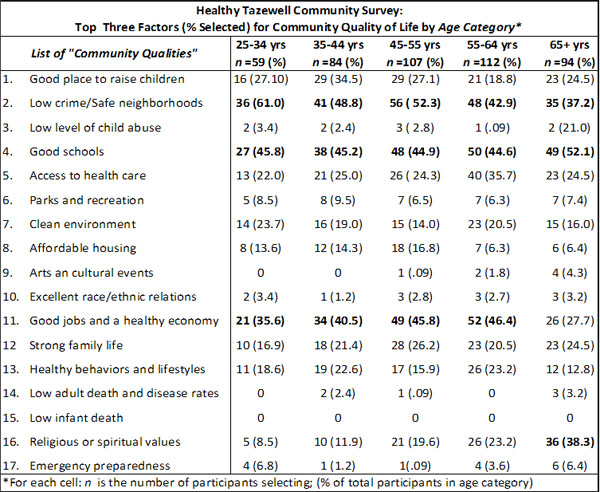
Community Quality of Life. The survey included 17 "community qualities" and participants were asked to select their top three qualities. The 17 are listed in Table 1, in addition to the number of individuals (and percentage) in each age category selecting that particular quality. For example, 56 participants (52.3 %) of the 45-55 year old category (n=107) selected "low crime/sage neighborhoods as one of their top three qualities of community life.
Table 1
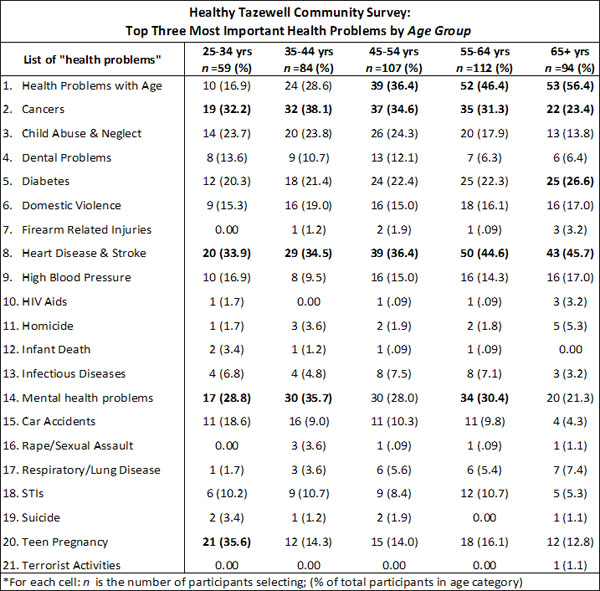
Health Problems. The survey included 21 "health or health related problems" and participants were asked to select the top three most important ones. The 21 are listed in Table 2, in addition to the number of individuals (and percentage) in each age category selecting that particular problem. For example, 21 participants (35.6%) of the 25-34 year old category (n=59) selected "teen pregnancy" as one of their top three health problems for the community.
Table 2
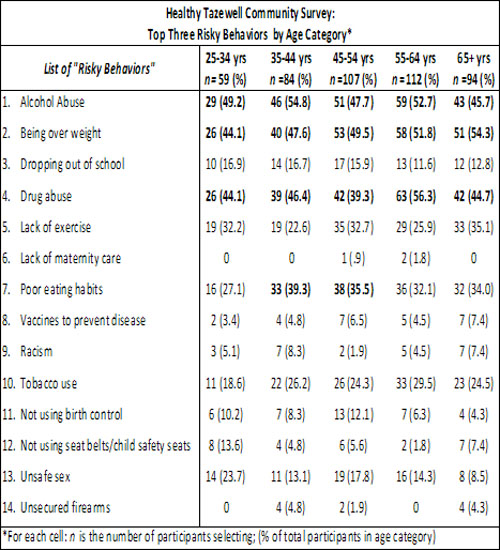
Risky Behaviors. The survey included 14 "risky behaviors" and participants were asked to select their top three behaviors. The 14 are listed in Table 3, in addition to the number of individuals (and percentage) in each age category selecting that particular risky behavior. For example, 51 participants (54.3%) of the 65 and over category (n=94) selected "being overweight" as one of their top three risky behaviors.
Table 3
Data Analysis
For this descriptive study, using SPSS 19.0, we ran frequency analyses for each listed option (i.e., Community Quality of Life, Health Problems, and Risky Behaviors) by age category. Ranking of the top three was based strictly on number of responses and corresponding percentages by age category.
Results
Community Quality of Life (Table 1). Overall, each age category listed the same three top qualities (low crime/safe neighborhoods, good schools, and good jobs/healthy economy). However, those in the 65 years of age and over category did not list "good jobs/healthy economy" but rather "religious or spiritual values" as one of their top three.
Health Problems (Table 2). All age categories listed "heart disease & stroke" in their top three health problems. Three of the five age categories (45-55 years, 55-64 years, and 65 years and older) listed "health problems with age" as one of their top three whereas four age categories (not including those 65 years and older) listed "cancers" as one of their top three health problems. Uniquely, respondents 25-34 years of age listed teen pregnancy as an important health problem (the top category for this age group listed this problem - 21 or 35.6% of the 59 category total); respondents 35-44 years of age listed "mental health problems" (n=30 or 35.7% of the 84 participants); and 25 or 26.6 percent of those 65 and over listed diabetes.
Risky Behaviors (Table 3). All age categories agreed that alcohol abuse, overweight, and drug abuse were the top three risky behaviors in the community.
Discussion
This study investigated the effect of age on the factors an individual associates with a healthy community. Due to the fact that age commonly causes variations in perception, it was hypothesized that the top factors for community quality of life, health problems, and risky behaviors would vary based on the age of the participant. Overall, results were mixed.
First, for quality of life, the age groups almost completely agreed: low crime/safe neighborhoods, good schools, and a healthy economy were nominated. However, the 65 and over age category did not list good jobs/healthy economy, but listed religious or spiritual values as a key factor for community quality of life. A large percentage of the 65 and older population is retired; only 36 percent of men, and 26 percent of women ages 65-69 are still in the workforce. This may contribute to a lower concern for good jobs and economic affairs compared to other age groups (Jacobsen, Kent, Lee, & Mather, 2011). In addition, there is often an increase in stress and loss that comes with increasing age (Hall, 1985). Religion can serve as a stress release and support system, while also giving guidance and providing social interaction; these are critical aspects, which may otherwise be lacking from an older adult's everyday life (Hall, 1985). In contrast, there is generally less interest and involvement in religion and spirituality from younger generations (Mason, Singleton, & Webber, 2007). However, views on life after death and a doctrine of right vs. wrong closely match those found in older adults, and rates of religious affiliation in those ages 18-29 closely match older generations during this stage of life (Pond, Smith, & Clement, 2010). As a result, it is thought that increased religious emphasis occurs with increases in age, and is thus age dependent.
Secondly, all age categories listed heart disease and stroke as a top health problem, while 45-55, 55-64, and over 65 listed health problems with aging, and all age groups but the over 65 group listed cancer. However, the youngest age group listed teen pregnancy as a top health concern. This age category also listed alcohol abuse, a known correlate of teenage pregnancy, along with other drug use, as a top risky behavior. A 2005 a study done by the CDC reported that of the 33.9 percemt sexually active teens, 23.3 percent reported using drugs or alcohol (CDC, 2011). In addition, Cavazos-Rehg and colleagues (2012) recently reported on the association of pregnancy by age 15 with cigarette and/or marijuana use. These findings are consistent with ours: alcohol, drug use, and teenage pregnancy are important risky behaviors to consider jointly in public health.
Lastly, the top three risky behaviors were consistent across all age categories, with all groups listing alcohol abuse, being over weight, and drug abuse. However, based on generational differences of health concern it was predicated that risky behaviors would also differ based on age cohort. This deviation may be from a lack of external validity within our sample. As mentioned previously, the above stated risky behaviors are linked to many of the top health problems listed by respondents. It's been determined that health literacy is highly dependent upon educational status (Rudd, 2007). Of our respondents, 61 percent held a college degree or higher, thus indicating the possibility of preexisting information in these subjects, and a higher level of knowledge, which may be an inconsistent representation of the total population (Oates, 2012).
Consequently, our study had several limitations. First, because of possible geographic differences in community health, our study may have limited generalizability for other community populations. Secondly, survey responses and demographics in our study warranted questionable external validity. Although 61 percent of our respondents held a college degree or higher, less than 24 percent of Tazewell County residents hold a bachelors degree (U.S. Census Bureau, 2013). In addition, 39.5 percent of survey responders indicated an annual household income over $70,000, compared to the county's median household income of $54,617 (U.S. Census Bureau, 2013). Thus, our information may not accurately represent Tazewell County as a whole.
This research has important implication for future research and public policy in Tazewell County. Future research will want to explore the definition and importance of religious or spiritual values with participants from each age category for clarification. Millennials, or those born between 1981 and 2003, have been shown to have less religious affiliation, and place lower importance on religion in everyday life compared to older generations (Pond, Smith & Clement, 2010). Younger generations may be religiously unaffiliated, practice a form of non-organized spirituality, or simply acknowledge the belief in a higher power, which could be inconsistent with predetermined definitions of religion (Mason, Singleton, & Webber, 2007; Pond, Smith & Clement, 2010). In addition, further consideration of preventive interventions for teen childbearing should also be investigated (Shearer, Gyaben, Gallagher, & Klerman, 2005).
References
Bakes-Martin, R., Corso, L. C., Landrum, L. B., Fischer, V. S., & Halverson, P. K. (2005). Developing national performance standards for local public health systems. Journal of Public Health Management Practice, 11 (5), 418-421.
Cavazos-Rehg, P. A., Krauss, M. J., Spitznagel, E. L., Schootman, M., Cottler, L. B., & Bierut, L. J. (2012). Brief report: Pregnant by age 15 years and substance use initiation among US adolescent girls. Journal of Adolescence, 35(5), 1393-1397.
Centers for Disease Control and Prevention. [CDC]. MMWR 2012; 61. Retrieved from http://www.cdc.gov/mmwr/pdf/ss/ss6104.pdf
DiClemente, R. J., Crosby, R. A., & Kegler, M. C. (2009). Emerging theories in health promotion, practice and research. San Francisco CA: Jossey-Bass
Hall, M. (1985). Religion and aging. Journal of Religion and Health, 24 (1), 70-78.
Israel, B. A., Schultz, A. J., Parker, E. A., & Becker, A. B. (1998). Review of community-based public health research: assessing partnership approaches to improve public health. Annual Review of Public Health, 19. Retrieved from http://depts.washington.edu/ccph/pdf_files/annurev.publhealth.19.1.pdf
Jacobsen, L.A., Kent, M., Lee, M., & Mather, M. (2011). America's aging population. Population Reference Bureau, 66 (1). Retrieved from http://www.prb.org/pdf11/aging-in-america.pdf
Mason, M., Singleton, A., & Webber, R. (2008). The spirit of Generation Y: Young people's spirituality in a changing Australia (12). Retrieved from https://dlibrary.acu.edu.au/research/ccls/sppub/071005_Summary_--_Key_Findings.pdf
McClellan, C. S. (2005). Utilizing a national performance standards local and public health assessment instrument in a community assessment process: the Clarendon County turning point initiative. Journal of Public Health Management Practice, 11 (5), 428-432.
Montepare, J. M. (2009). Subjective age: Toward a guiding lifespan framework. International Journal of Behavioral Development, 33 (1), 42-46.
Norris, T., & Pittman, M. (2000). The healthy communities movement and the coalition for healthier cities and communities. Public Health Reports, 115. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1308699/
Pond, A., Smith, G., Clement, S. (2010). Religion among the Millenials: Less religiously active than older Americans but fairly traditional in other ways. Pew Research Center. Retrieved from http://www.pewforum.org/files/2010/02/millennials-report.pdf
Oates, E., Cluskey, M., & Randall, G. K. (2012). Healthy Tazewell County initiative: Implementation of the MAPP process and survey findings. Undergraduate Research Journal for the Human Sciences, 11. Retrieved from /urc/v11/oates.html
Rudd, R. E. (2007). Health literacy skills of U.S. adults. American Journal of Health Behavior,31. Retrieved from http://www.chpcp.org/servicecoord/chronicdisease/HealthLit/Health%20Literacy%20Skills%20of%20US%20Adults.pdf
Shearer, D. L., Gyaben, S. L., Gallagher, K. M., & Klerman, L. V. (2005). Selecting, implementing, and evaluating teen pregnancy prevention interventions: Lessons from the CDC's Community Coalition Partnership Programs for the Prevention of Teen Pregnancy. Journal of Adolescent Health, 37(3), Supplement, S42-S52.
Stover, G. N., & Bassett, M. T. (2003). Practice is the purpose of public health. American Journal of Public Health, 93. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1448052/
U.S. Department of Commerce, United States Census Bureau (2013). Retrieved from http://quickfacts.census.gov/qfd/states/17/17179.html
U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. (2011). Youth Risk Behavior Surveillance. Morbidity and Mortality Weekly Report, 64 (4). Retrieved from http://www.cdc.gov/mmwr/pdf/ss/ss6104.pdf
|